Showcasing the process for building a multi-hop retrieval system using DSPy and Indexify
TLDR;
- In this article, we will explore multi-hop retrieval and how it can be leveraged to build RAG systems that require complex reasoning
- We will see the technique by building a Q&A chatbot in the healthcare domain using Indexify, OpenAI, and DSPy.
- How the multi-hop chain-of-thought RAG efficiently answers complex questions.
Introduction
Retrieval-Augmented Generation (RAG) systems have emerged as a powerful approach to building LLM-powered applications. RAG systems operate by first retrieving information from external knowledge sources using a retrieval model, and then using this information to prompt LLMs to generate responses.
However, a basic RAG system (also known as naive RAG) may face challenges when dealing with complex queries that require reasoning over multiple pieces of information. This is where multi-hop retrieval comes into play.
In multi-hop retrieval, the system gathers information across multiple steps or “hops” to answer complex questions or gather detailed information. This technique is common in advanced question-answering systems, where multiple sources or documents contain the necessary information to answer a question.
Building a multi-hop retrieval is a key challenge in natural language processing (NLP) and information retrieval because it requires the system to understand the relationships between different pieces of information and how they contribute to the overall answer.
In this article, my goal is to showcase the process for building a multi-hop retrieval system using DSPy and Indexify. I will use the technique in a RAG system for the healthcare domain, and demonstrate how it improves response quality.
What Is Multi-Hop Retrieval?
To understand multi-hop retrieval better, let’s look at one example first.
Note that the retrieval step below does not have access to the Internet and is dependent on the context you provide.
Suppose you have a query: “Who was the captain of India in the T20 World Cup 2024 co-hosted by the West Indies and the United States?”
Let’s say we feed this question to a vector database, and we get two nearest matching context passages that can solve this question:
“After Virat Kohli stepped down as India’s T20 captain in 2021 following the unsuccessful 20-over World Cup format, the animosity between…”
And
“Rohit Sharma has been named the new captain of India’s T20 side, replacing Virat Kohli, the cricket board said after the side was dumped out …”
Nowhere in these two passages is it mentioned exactly who was captain of the team in the 2024 World Cup, but if we were to choose one, we would answer “Rohit Sharma” since:
1. Virat Kohli stepped down in 2021, and
2. Rohit Sharma took over as the new captain.
So, it’s highly likely that Rohit Sharma is still the captain in 2024. Again, based on the available context, one could say we had to hop two times before reaching the answer.
This logical thinking is normal to us since we are humans, but it’s a big task for machine learning models. Thanks to LLMs, we can now easily solve such questions using multi-hop retrieval.

Some applications of multi-hop retrieval include:
- Healthcare Bots: Finding and querying over patients’ admission data.
- Text Summarizers: Summarizing large amounts of text efficiently.
- Question-Answering Bots: Providing answers to various types of queries.
- Legal Industry: Creating a retrieval model for legal cases.
- HR Industry: Finding perfect candidates for a job by matching certain filters.
Problem Statement
In this experiment, I will build a Multi-Hop Question-Answering chatbot using Indexify, OpenAI, and DSPy (a Declarative Sequencing Python framework). DSPy is a framework that enables declarative programming of language models (LMs), replacing traditional prompting with composable modules. The framework is extremely useful for building LLM-powered applications that involve complex reasoning.
Architecture Overview
Indexify
Indexify is a highly scalable data framework designed to build ingestion and extraction pipelines for unstructured data. These pipelines are defined using declarative configuration. Each stage of the pipeline can perform structured extraction using any AI model or transform ingested data. The pipelines start working immediately upon data ingestion into Indexify, making them ideal for interactive applications and low-latency use cases.
Indexify solves a major problem affecting RAG systems: scalable and predictable parsing of unstructured data.
OpenAI
We will be using OpenAI’s API to generate responses. You can also use their APIs if you have an account with them. Head on to: OpenAI Platform.
DSPy
DSPy is a framework for algorithmically optimizing Language Model prompts instead of manually prompting. If you look at their GitHub, you will see that they mention “Programming — not prompting”. How did they achieve this? With the help of Signatures, Modules, Metrics and Optimizers. To know more about DSPy, read the paper “DSPy: Compiling Declarative Language Model Calls into Self-Improving Pipelines” by Omar Khattab et al.
Dataset
For this experiment, I will use the Wikipedia Healthcare Terms dataset from Hugging Face. Check it out here: gamino/wiki_medical_terms (GPL 3.0 license).

Code Setup
OS preferred: Linux. If you have Windows or macOS, try to run this with the Linux build tools.
Before starting up, let’s install the required packages:
!pip install indexify-dspy
!pip install indexify
!pip install indexify-extractor-sdk
!pip install gradio==4.31.0
To test whether the packages have been installed correctly:
import dspy
from indexify import IndexifyClient
from indexify_dspy.retriever import IndexifyRM
If you are facing issues like ModuleError: “dspy not found”, you can install this particular version and try to see if it resolves the issue:
!pip install dspy-ai==2.0.8
Data Ingestion Using Indexify
Before we start the Indexify servers, let’s look at the dataset:
import pandas as pd
df = pd.read_parquet("hf://datasets/gamino/wiki_medical_terms/wiki_medical_terms.parquet")
df=df.dropna()
print(df)
Which gives:
We have two columns, page_title and page_text. We will use page_text.
medical_descriptions = df['page_text'].tolist()
Now that we are done with the dataset let’s start Indexify’s Server and Extractors.
To start the server, open a terminal and type:
$ curl https://getindexify.ai | sh
$ ./indexify server -d
(These are two separate lines.)
Open a second terminal, and to download and start the extractors, use:
$ indexify-extractor download tensorlake/minilm-l6
$ indexify-extractor download tensorlake/chunk-extractor
$ indexify-extractor join-server
After these two terminals are up and running, let’s ingest the medical_descriptions:
from indexify import IndexifyClient, ExtractionGraph
indexify_client = IndexifyClient()
extraction_graph_spec = """
name: 'medical'
extraction_policies:
- extractor: 'tensorlake/minilm-l6'
name: 'minilml6'
"""
extraction_graph = ExtractionGraph.from_yaml(extraction_graph_spec)
indexify_client.create_extraction_graph(extraction_graph)
indexify_client.add_documents(
"medical",
medical_descriptions,
)
It took me about 30 seconds to ingest 7,000 records! Pretty fast!
Now that we have created our client let’s use DSPy integration for Indexify and try to see how it retrieves the top k contexts:
def generate_context(query, k):
retrieve = IndexifyRM(indexify_client)
topk_passages = retrieve(query, "medical.minilml6.embedding", k=k).passages
return topk_passages
For example, take this query:
query = "heart attack"
generate_context(query=query, k=2)
Which gives:
['Carditis (pl. carditides) is the inflammation of the heart. It is usually studied and treated by specifying it as:nPericarditis is the inflammation of the pericardiumnMyocarditis is the inflammation of the heart musclenEndocarditis is the inflammation of the endocardiumnPancarditis, also called perimyoendocarditis, is the inflammation of the entire heart: the pericardium, the myocardium and the endocardiumnReflux carditis refers to a possible outcome of esophageal reflux (also known as GERD), and involves inflammation of the esophagus/stomach mucosannn== References ==',
'Coronary artery disease (CAD), also called coronary heart disease (CHD), ischemic heart disease (IHD), myocardial ischemia, or simply heart disease, involves the reduction of blood flow to the heart muscle due to build-up of atherosclerotic plaque in the arteries of the heart. It is the most common of the cardiovascular diseases. Types include stable angina, unstable angina, myocardial infarction, and sudden cardiac death. A common symptom is chest pain or discomfort which may travel into the shoulder, arm, back, neck, or jaw. Occasionally it may feel like heartburn. Usually symptoms occur with exercise or emotional stress, last less than a few minutes, and improve with rest. Shortness of breath may also occur and sometimes no symptoms are present. In many cases, the first sign is a heart attack. Other complications include heart failure or an abnormal heartbeat.Risk factors include high blood pressure, smoking, diabetes, lack of exercise, obesity, high blood cholesterol, poor diet, depression, and excessive alcohol consumption. A number of tests may help with diagnoses including: electrocardiogram, cardiac stress testing, coronary computed tomographic angiography, and coronary angiogram, among others.Ways to reduce CAD risk include eating a healthy diet, regularly exercising, maintaining a healthy weight, and not smoking. Medications for diabetes, high cholesterol, or high blood pressure are sometimes used. There is limited evidence for screening people who are at low risk and do not have symptoms. Treatment involves the same measures as prevention. Additional medications such as antiplatelets (including aspirin), beta blockers, or nitroglycerin may be recommended. Procedures such as percutaneous coronary intervention (PCI) or coronary artery bypass surgery (CABG) may be used in severe disease. In those with stable CAD it is unclear if PCI or CABG in addition to the other treatments improves life expectancy or decreases heart attack risk.In 2015, CAD affected 110 million people and resulted in 8.9 million deaths. It makes up 15.6% of all deaths, making it the most common cause of death globally. The risk of death from CAD for a given age decreased between 1980 and 2010, especially in developed countries. The number of cases of CAD for a given age also decreased between 1990 and 2010. In the United States in 2010, about 20% of those over 65 had CAD, while it was present in 7% of those 45 to 64, and 1.3% of those 18 to 45; rates were higher among men than women of a given age.nnSigns and symptomsnThe narrowing of coronary arteries reduces the supply of oxygen-rich blood flowing to the heart, which becomes more pronounced during strenuous activities during which the heart beats faster. For some, this causes severe symptoms, while others experience no symptoms at all. The most common symptom is chest pain or discomfort that occurs regularly with activity, after eating, or at other predictable times;]
Above, Indexify has removed the headache of parsing PDFs, generating embeddings, and querying with them.
This is powerful because one of the biggest failure points of RAG systems is noise in the data. When we take any unstructured document, say a PDF or HTML, and use a standard parser, it leaves several artifacts in the final text that confuse the embedding generation process.
With Indexify, we have removed leftover artifacts using a drop-in solution. Their documentation explains the engine’s capabilities.
Multi-Hop Chain-of-Thought RAG with DSPy
Let’s create a class RAGSignature and define three input fields:
- Context: The context for a query to be used by the LLM.
- Question: The query the user will ask.
- Answer: The answer to the query.
Notice how I have defined the descriptions in the context and the answer; interestingly, DSPy uses this description while building the pipeline, ensuring it’s semantically correct to get the best results.
class RAGSignature(dspy.Signature):
"""Answer questions based on given the context."""
context = dspy.InputField(desc="may contain relevant facts")
question = dspy.InputField()
answer = dspy.OutputField(desc="an answer not more than 1 paragraph")
Since multi-hop systems try to break the question into several manageable questions to create parts of the questions, we will use another signature that will generate queries from the question:
class GenerateSearchQuery(dspy.Signature):
"""Write a simple search query that will help answer a complex question."""
context = dspy.InputField(desc="may contain relevant facts")
question = dspy.InputField()
query = dspy.OutputField()
Now, finally, let’s build the MultiHopChainOfThoughtRAG class, which essentially tries to:
- Create a dynamic query generator that will run max_hops times, meaning we can define how many hops the model should take before arriving at the answer.
- Each time, we feed the generated query into our Indexify context extractor and get the context to answer that generated query. We do this max_hops times, and finally, we get the final context that has the contexts for all the generated queries.
- Lastly, we deduplicate the context to remove duplicate context entities.
In this way, we can answer each part of the question gracefully.
from dsp.utils import deduplicate
class MultiHopChainOfThoughtRAG(dspy.Module):
def __init__(self, passages_per_hop=3, max_hops=2):
super().__init__()
self.generate_query = [dspy.ChainOfThought(GenerateSearchQuery) for _ in range(max_hops)]
self.retrieve = dspy.Retrieve(k=passages_per_hop)
self.generate_answer = dspy.ChainOfThought(RAGSignature)
self.max_hops = max_hops
self.k = passages_per_hop
def forward(self, question):
context = []
for hop in range(self.max_hops):
query = self.generate_query[hop](context=context, question=question).query
passages = generate_context(query, k=self.k)
context = deduplicate(context + passages)
pred = self.generate_answer(context=context, question=question)
return dspy.Prediction(context=context, answer=pred.answer)
It’s time to test our Multi-Hop RAG.
Results
Now that we have done the hard part, let’s see the results.
Query: Does overdosing on paracetamol cause kidney failure? If I consume 3 grams at once, is it an overdose?
query = "Does overdosing on paracetamol cures kidney failure? If I consume 3 grams at once, is it an overdose?"
response = multi_hop_rag(query).answer
print(response)
Answer:
Overdosing on paracetamol does not cause kidney failure, and taking 3 grams at once is not considered an overdose for a healthy adult.
Let’s see what’s happening in the background using:
turbo.inspect_history(1)
Answer questions based on the given context.
---
Follow the following format.
Context: may contain relevant facts
Question: ${question}
Reasoning: Let's think step by step in order to ${produce the answer}. We ...
Answer: an answer not more than 2 lines
---
Context:
«Paracetamol poisoning, also known as acetaminophen poisoning, is caused by excessive use of the medication paracetamol (acetaminophen). Most people have few or non-specific symptoms in the first 24 hours following overdose. These include feeling tired, abdominal pain, or nausea. This is typically followed by a couple of days without any symptoms, after which yellowish skin, blood clotting problems, and confusion occurs as a result of liver failure. Additional complications may include kidney failure, pancreatitis, low blood sugar, and lactic acidosis. If death does not occur, people tend to recover fully over a couple of weeks. Without treatment, death from toxicity occurs 4 to 18 days later.Paracetamol poisoning can occur accidentally or as an attempt to die by suicide. Risk factors for toxicity include alcoholism, malnutrition, and the taking of certain other hepatotoxic medications. Liver damage results not from paracetamol itself, but from one of its metabolites, N-acetyl-p-benzoquinone imine (NAPQI). NAPQI decreases the livers glutathione and directly damages cells in the liver. Diagnosis is based on the blood level of paracetamol at specific times after the medication was taken. These values are often plotted on the Rumack-Matthew nomogram to determine level of concern.Treatment may include activated charcoal if the person seeks medical help soon after the overdose. Attempting to force the person to vomit is not recommended. If there is a potential for toxicity, the antidote acetylcysteine is recommended. The medication is generally given for at least 24 hours. Psychiatric care may be required following recovery. A liver transplant may be required if damage to the liver becomes severe. The need for transplant is often based on low blood pH, high blood lactate, poor blood clotting, or significant hepatic encephalopathy. With early treatment liver failure is rare. Death occurs in about 0.1% of cases.Paracetamol poisoning was first described in the 1960s. Rates of poisoning vary significantly between regions of the world. In the United States more than 100,000 cases occur a year. In the United Kingdom it is the medication responsible for the greatest number of overdoses. Young children are most commonly affected. In the United States and the United Kingdom, paracetamol is the most common cause of acute liver failure.
Signs and symptoms
The signs and symptoms of paracetamol toxicity occur in three phases. The first phase begins within hours of overdose, and consists of nausea, vomiting, a pale appearance, and sweating. However, patients often have no specific symptoms or only mild symptoms in the first 24 hours of poisoning. Rarely, after massive overdoses, patients may develop symptoms of metabolic acidosis and coma early in the course of poisoning. The second phase occurs between 24 hours and 72 hours following overdose and consists of signs of increasing liver damage. In general, damage occurs in liver cells as they metabolize the paracetamol. The individual may experience right upper quadrant abdominal pain. The increasing liver damage also changes biochemical markers of liver function; International normalized ratio (INR) and the liver transaminases ALT and AST rise to abnormal levels. Acute kidney failure may also occur during this phase, typically caused by either hepatorenal syndrome or multiple organ dysfunction syndrome. In some cases, acute kidney failure may be the primary clinical manifestation of toxicity. In these cases, it has been suggested that the toxic metabolite is produced more in the kidneys than in the liver. The third phase follows at 3 to 5 days and is marked by complications of massive liver necrosis leading to fulminant liver failure with complications of coagulation defects, low blood sugar, kidney failure, hepatic encephalopathy, brain swelling, sepsis, multiple organ failure, and death. If the third phase is survived, the liver necrosis runs its course, and liver and kidney function typically return to normal in a few weeks. The severity of paracetamol toxicity varies depending on the dose and whether appropriate treatment is received.
Cause
The toxic dose of paracetamol is highly variable. In general the recommended maximum daily dose for healthy adults is 4 grams. Higher doses lead to increasing risk of toxicity. In adults, single doses above 10 grams or 200 mg/kg of bodyweight, whichever is lower, have a reasonable likelihood of causing toxicity. Toxicity can also occur when multiple smaller doses within 24 hours exceed these levels. Following a dose of 1 gram of paracetamol four times a day for two weeks, patients can expect an increase in alanine transaminase in their liver to typically about three times the normal value. It is unlikely that this dose would lead to liver failure. Studies have shown significant hepatotoxicity is uncommon in patients who have taken greater than normal doses over 3 to 4 days. In adults, a dose of 6 grams a day over the preceding 48 hours could potentially lead to toxicity, while in children acute doses above 200 mg/kg could potentially cause toxicity. Acute paracetamol overdose in children rarely causes illness or death, and it is very uncommon for children to have levels that require treatment, with chronic larger-than-normal doses being the major cause of toxicity in children.Intentional overdosing (self-poisoning, with suicidal intent) is frequently implicated in paracetamol toxicity. In a 2006 review, paracetamol was the most frequently ingested compound in intentional overdosing.In rare individuals, paracetamol toxicity can result from normal use. This may be due to individual ("idiosyncratic") differences in the expression and activity of certain enzymes in one of the metabolic pathways that handle paracetamol (see paracetamols metabolism).
Risk factors
A number of factors can potentially increase the risk of developing paracetamol toxicity. Chronic excessive alcohol consumption can induce CYP2E1, thus increasing the potential toxicity of paracetamol. In one study of patients with liver injury, 64% reported alcohol intakes of greater than 80 grams a day, while 35% took 60 grams a day or less. Whether chronic alcoholism should be considered a risk factor has been debated by some clinical toxicologists. For chronic alcohol users, acute alcohol ingestion at the time of a paracetamol overdose may have a protective effect. For non-chronic alcohol users, acute alcohol consumption had no protective effect.
Fasting is a risk factor, possibly because of depletion of liver glutathione reserves. The concomitant use of the CYP2E1 inducer isoniazid increases the risk of hepatotoxicity, though whether 2E1 induction is related to the hepatotoxicity in this case is unclear. Concomitant use of other drugs that induce CYP enzymes, such as antiepileptics including carbamazepine, phenytoin, and barbiturates, have also been reported as risk factors.
Pathophysiology
When taken in normal therapeutic doses, paracetamol has been shown to be safe. Following a therapeutic dose, it is mostly converted to nontoxic metabolites via Phase II metabolism by conjugation with sulfate and glucuronide, with a small portion being oxidized via the cytochrome P450 enzyme system. Cytochromes P450 2E1 and 3A4 convert approximately 5% of paracetamol to a highly reactive intermediary metabolite, N-acetyl-p-benzoquinone imine (NAPQI). Under normal conditions, NAPQI is detoxified by conjugation with glutathione to form cysteine and mercapturic acid conjugates.In cases of paracetamol overdose, the sulfate and glucuronide pathways become saturated, and more paracetamol is shunted to the cytochrome P450 system to produce NAPQI. As a result, hepatocellular supplies of glutathione become depleted, as the demand for glutathione is higher than its regeneration. NAPQI therefore remains in its toxic form in the liver and reacts with cellular membrane molecules, resulting in widespread hepatocyte damage and death, leading to acute liver necrosis. In animal studies, the livers stores of glutathione must be depleted to less than 70% of normal levels before liver toxicity occurs.
Diagnosis
A persons history of taking paracetamol is somewhat accurate for the diagnosis. The most effective way to diagnose poisoning is by obtaining a blood paracetamol level. A drug nomogram developed in 1975, called the Rumack-Matthew nomogram, estimates the risk of toxicity based on the serum concentration of paracetamol at a given number of hours after ingestion. To determine the risk of potential hepatotoxicity, the paracetamol level is traced along the nomogram. Use of a timed serum paracetamol level plotted on the nomogram appears to be the best marker indicating the potential for liver injury. A paracetamol level drawn in the first four hours after ingestion may underestimate the amount in the system because paracetamol may still be in the process of being absorbed from the gastrointestinal tract. Therefore, a serum level taken before 4 hours is not recommended.Clinical or biochemical evidence of liver toxicity may develop in one to four days, although, in severe cases, it may be evident in 12 hours. Right-upper-quadrant tenderness may be present and can aid in diagnosis. Laboratory studies may show evidence of liver necrosis with elevated AST, ALT, bilirubin, and prolonged coagulation times, particularly an elevated prothrombin time. After paracetamol overdose, when AST and ALT exceed 1000 IU/L, paracetamol-induced hepatotoxicity can be diagnosed. In some cases, the AST and ALT levels can exceed 10,000 IU/L.
Detection in body fluids
Paracetamol may be quantified in blood, plasma, or urine as a diagnostic tool in clinical poisoning situations or to aid in the medicolegal investigation of suspicious deaths. The concentration in serum after a typical dose of paracetamol usually peaks below 30 mg/L, which equals 200 μmol/L. Levels of 30-300 mg/L (200-2000 μmol/L) are often observed in overdose patients. Postmortem blood levels have ranged from 50 to 400 mg/L in persons dying due to acute overdosage. Automated colorimetric techniques, gas chromatography and liquid chromatography are currently in use for the laboratory analysis of the drug in physiological specimens.
Prevention
Limitation of availability
Limiting the availability of paracetamol tablets has been attempted in some countries. In the UK, sales of over-the-counter paracetamol are restricted to packs of 32 x 500 mg tablets in pharmacies, and 16 x 500 mg tablets in non-pharmacy outlets. Pharmacists may provide up to 100 tablets for those with chronic conditions at the pharmacists discretion. In Ireland, the limits are 24 and 12 tablets, respectively. Subsequent study suggests that the reduced availability in large numbers had a significant effect in reducing poisoning deaths from paracetamol overdose.One suggested method of prevention is to make paracetamol a prescription-only medicine, or to remove it entirely from the market. However, overdose is a relatively minor problem; for example, 0.08% of the UK population (over 50 thousand people) present with paracetamol overdose each year. In contrast, paracetamol is a safe and effective medication that is taken without complications by millions of people. In addition, alternative pain relief medications such as aspirin are more toxic in overdose, whereas non-steroidal anti-inflammatory drugs are associated with more adverse effects following normal use.
Combination with other agents
One strategy for reducing harm done by acetaminophen overdoses is selling paracetamol pre-combined in tablets either with an emetic or an antidote. Paradote was a tablet sold in the UK which combined 500 mg paracetamol with 100 mg methionine, an amino acid formerly used in the treatment of paracetamol overdose.
There have been no studies so far on the effectiveness of paracetamol when given in combination with its most commonly used antidote, acetylcysteine.Calcitriol, the active metabolite of vitamin D3, appears to be a catalyst for glutathione production. Calcitriol was found to increase glutathione levels in rat astrocyte primary cultures on average by 42%, increasing glutathione protein concentrations from 29 nmol/mg to 41 nmol/mg, 24 and 48 hours after administration; it continued to have an influence on glutathione levels 96 hours after administration. It has been proposed that co-administration of calcitriol, via injection, may improve treatment outcomes.
Paracetamol replacements
Paracetamol ester prodrug with L-pyroglutamic acid (PCA), a biosynthetic precursor of glutathione, has been synthesized to reduce paracetamol hepatotoxicity and improve bioavailability. The toxicological studies of different paracetamol esters show that L-5-oxo-pyrrolidine-2-paracetamol carboxylate reduces toxicity after administration of an overdose of paracetamol to mice. The liver glutathione values in mice induced by intraperitoneal injection of the ester are superimposable with the GSH levels recorded in untreated mice control group. The mice group treated with an equivalent dose of paracetamol showed a significative decrease of glutathione of 35% (p<0.01 vs untreated control group). The oral LD50 was found to be greater than 2000 mg kg-1, whereas the intraperitoneal LD50 was 1900 mg kg-1. These results taken together with the good hydrolysis and bioavailability data show that this ester is a potential candidate as a prodrug of paracetamol.
Treatment
Gastric decontamination
In adults, the initial treatment for paracetamol overdose is gastrointestinal decontamination. Paracetamol absorption from the gastrointestinal tract is complete within two hours under normal circumstances, so decontamination is most helpful if performed within this timeframe. Gastric lavage, better known as stomach pumping, may be considered if the amount ingested is potentially life-threatening and the procedure can be performed within 60 minutes of ingestion. Activated charcoal is the most common gastrointestinal decontamination procedure as it adsorbs paracetamol, reducing its gastrointestinal absorption. Administering activated charcoal also poses less risk of aspiration than gastric lavage.It appears that the most benefit from activated charcoal is gained if it is given within 30 minutes to two hours of ingestion. Administering activated charcoal later than 2 hours can be considered in patients that may have delayed gastric emptying due to co-ingested drugs or following ingestion of sustained- or delayed-release paracetamol preparations. Activated charcoal should also be administered if co-ingested drugs warrant decontamination. There was reluctance to give activated charcoal in paracetamol overdose, because of the concern that it may also absorb the oral antidote acetylcysteine. Studies have shown that 39% less acetylcysteine is absorbed into the body when they are administered together. There are conflicting recommendations regarding whether to change the dosing of oral acetylcysteine after the administration of activated charcoal, and even whether the dosing of acetylcysteine needs to be altered at all. Intravenous acetylcysteine has no interaction with activated charcoal.
Inducing vomiting with syrup of ipecac has no role in paracetamol overdose because the vomiting it induces delays the effective administration of activated charcoal and oral acetylcysteine. Liver injury is extremely rare after acute accidental ingestion in children under 6 years of age. Children with accidental exposures do not require gastrointestinal decontamination with either gastric lavage, activated charcoal, or syrup of ipecac.
Acetylcysteine
Acetylcysteine, also called N-acetylcysteine or NAC, works to reduce paracetamol toxicity by replenishing body stores of the antioxidant glutathione. Glutathione reacts with the toxic NAPQI metabolite so that it does not damage cells and can be safely excreted. NAC was usually given following a treatment nomogram (one for patients with risk factors, and one for those without) but the use of the nomogram is no longer recommended as the evidence base to support the use of risk factors was poor and inconsistent and many of the risk factors are imprecise and difficult to determine with sufficient certainty in clinical practice. Cysteamine and methionine have also been used to prevent hepatotoxicity, although studies show that both are associated with more adverse effects than acetylcysteine. Additionally, acetylcysteine has been shown to be a more effective antidote, particularly in patients presenting greater than 8 hours post-ingestion and for those who present with liver failure symptoms.If the person presents less than eight hours after paracetamol overdose, then acetylcysteine significantly reduces the risk of serious hepatotoxicity and guarantees survival. If acetylcysteine is started more than 8 hours after ingestion, there is a sharp decline in its effectiveness because the cascade of toxic events in the liver has already begun, and the risk of acute liver necrosis and death increases dramatically. Although acetylcysteine is most effective if given early, it still has beneficial effects if given as late as 48 hours after ingestion. If the person presents more than eight hours after the paracetamol overdose, then activated charcoal is not useful, and acetylcysteine is started immediately. In earlier presentations, charcoal can be given when the patient arrives and acetylcysteine is initiated while waiting for the paracetamol level results to return from the laboratory.In United States practice, intravenous (IV) and oral administration are considered to be equally effective and safe if given within 8 hours of ingestion. However, IV is the only recommended route in Australasian and British practice. Oral acetylcysteine is given as a 140 mg/kg loading dose followed by 70 mg/kg every four hours for 17 more doses, and if the patient vomits within 1 hour of dose, the dose must be repeated. Oral acetylcysteine may be poorly tolerated due to its unpleasant taste, odor, and its tendency to cause nausea and vomiting. If repeated doses of charcoal are indicated because of another ingested drug, then subsequent doses of charcoal and acetylcysteine should be staggered.Intravenous acetylcysteine is given as a continuous infusion over 20 hours for a total dose 300 mg/kg. Recommended administration involves infusion of a 150 mg/kg loading dose over 15 to 60 minutes, followed by a 50 mg/kg infusion over four hours; the last 100 mg/kg are infused over the remaining 16 hours of the protocol. Intravenous acetylcysteine has the advantage of shortening hospital stay, increasing both doctor and patient convenience, and allowing administration of activated charcoal to reduce absorption of both the paracetamol and any co-ingested drugs without concerns about interference with oral acetylcysteine. Intravenous dosing varies with weight, specifically in children. For patients less than 20 kg, the loading dose is 150 mg/kg in 3 mL/kg diluent, administered over 60 minutes; the second dose is 50 mg/kg in 7 mL/kg diluent over 4 hours; and the third and final dose is 100 mg/kg in 14 mL/kg diluent over 16 hours.The most common adverse effect to acetylcysteine treatment is an anaphylactoid reaction, usually manifested by rash, wheeze, or mild hypotension. May cause infertility or death. Adverse reactions are more common in people treated with IV acetylcysteine, occurring in up to 20% of patients. Anaphylactoid reactions are more likely to occur with the first infusion (the loading dose). Rarely, severe life-threatening reactions may occur in predisposed individuals, such as patients with asthma or atopic dermatitis, and may be characterized by respiratory distress, facial swelling, and even death.If an anaphylactoid reaction occurs the acetylcysteine is temporarily halted or slowed and antihistamines and other supportive care is administered. For example, a nebulised beta-agonist like salbutamol may be indicated in the event of significant bronchospasm (or prophylactically in patients with a history of bronchospasm secondary to acetylcysteine). It is also important to closely monitor fluids and electrolytes.
Liver transplant
In people who develop acute liver failure or who are otherwise expected to die from liver failure, the mainstay of management is liver transplantation. Liver transplants are performed in specialist centers. The most commonly used criteria for liver transplant were developed by physicians at Kings College Hospital in London. Patients are recommended for transplant if they have an arterial blood pH less than 7.3 after fluid resuscitation or if a patient has Grade III or IV encephalopathy, a prothrombin time greater than 100 seconds, and a serum creatinine greater than 300 mmol/L In a 24-hour period. Other forms of liver support have been used including partial liver transplants. These techniques have the advantage of supporting the patient while their own liver regenerates. Once liver function returns immunosuppressive drugs are commenced and they have to take immunosuppressive medication for the rest of their lives.
Prognosis
The mortality rate from paracetamol overdose increases two days after the ingestion, reaches a maximum on day four, and then gradually decreases. Acidosis is the most important single indicator of probable mortality and the need for transplantation. A mortality rate of 95% without transplant was reported in patients who had a documented pH less than 7.30. Other indicators of poor prognosis include chronic kidney disease (stage 3 or worse), hepatic encephalopathy, a markedly elevated prothrombin time, or an elevated blood lactic acid level (lactic acidosis). One study has shown that a factor V level less than 10% of normal indicated a poor prognosis (91% mortality), whereas a ratio of factor VIII to factor V of less than 30 indicated a good prognosis (100% survival). Patients with a poor prognosis are usually identified for likely liver transplantation. Patients that do not die are expected to fully recover and have a normal life expectancy and quality of life.
Epidemiology
Many over-the-counter and prescription-only medications contain paracetamol. Because of its wide availability paired with comparably high toxicity, (compared to ibuprofen and aspirin) there is a much higher potential for overdose. Paracetamol toxicity is one of the most common causes of poisoning worldwide. In the United States, the United Kingdom, Australia, and New Zealand, paracetamol is the most common cause of drug overdoses. Additionally, in both the United States and the United Kingdom it is the most common cause of acute liver failure.In England and Wales an estimated 41,200 cases of paracetamol poisoning occurred in 1989 to 1990, with a mortality of 0.40%. It is estimated that 150 to 200 deaths and 15 to 20 liver transplants occur as a result of poisoning each year in England and Wales. Paracetamol overdose results in more calls to poison control centers in the US than overdose of any other pharmacological substance, accounting for more than 100,000 calls, as well as 56,000 emergency room visits, 2,600 hospitalizations, and 458 deaths due to acute liver failure per year. A study of cases of acute liver failure between November 2000 and October 2004 by the Centers for Disease Control and Prevention in the USA found that paracetamol was the cause of 41% of all cases in adults, and 25% of cases in children.
References
External links
Gerth, Jeff; T. Christian Miller (September 20, 2013). "Use Only as Directed". ProPublica. Retrieved October 12, 2013.»
Question: does overdosing on paracetamol cures kidney failure? and what if i take 3 grams at once am i overdosing?
Reasoning: Let's think step by step in order to produce the answer. We know that paracetamol overdose can lead to liver failure, not kidney failure. Taking 3 grams of paracetamol at once is not considered an overdose for a healthy adult.
Answer: Overdosing on paracetamol does not cure kidney failure, and taking 3 grams at once is not considered an overdose for a healthy adult.
As you can see, the output is very impressive. Not only does our model know how to deal with fallacies, such as the notion that an overdose of paracetamol cures kidney failure, but it can also reason that up to 4 grams of paracetamol is not considered dangerous for adults. Thus, taking 3 grams is not an overdose.
We can even ask questions containing no commonality between the sub-questions, like:
Query: What is primary progressive aphasia and does it cause heart attacks? If not, what causes them?
query = "What is Primary progressive aphasia and does it cause heart attacks? If not, what causes them?"
response = multi_hop_rag(query).answer
print(response)
Answer:
Primary progressive aphasia is a type of neurological syndrome that impairs language capabilities. It does not cause heart attacks. Heart attacks are typically caused by cardiovascular diseases, such as atherosclerosis, high blood pressure, and other risk factors.
Pretty cool! Even though there’s no common context between PPA and heart attacks, our model can fetch the required context and answer confidently.
Creating a Simple UI Using Gradio
Let’s create a simple UI on top of our Multi-Hop RAG for better visual presentation.
import gradio as gr
with gr.Blocks() as demo:
chatbot = gr.Chatbot()
msg = gr.Textbox()
clear = gr.ClearButton([msg, chatbot])
def respond(query, chat_history):
response = multi_hop_rag(query)
chat_history.append((query, response.answer))
return "", chat_history
msg.submit(respond, [msg, chatbot], [msg, chatbot])
To start the Gradio server, use:
demo.launch(share=True)
# demo.launch(share=True) if using colab
# demo.close() to close the server
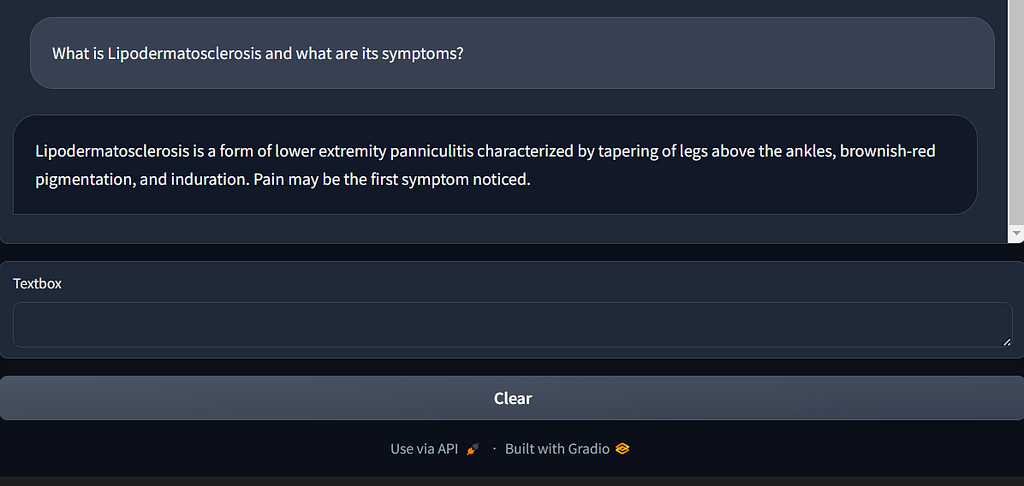
Query: What is Lipodermatosclerosis and what are its symptoms?
Key Takeaways
- In this article, we saw one of the applications of Indexify using DSPy.
- We built a multi-hop chain-of-thought RAG from scratch and saw how efficiently it answers questions.
GitHub
For the full code reference, please take a look at my repo:
https://github.com/sachink1729/DSPy-Multi-Hop-Chain-of-Thought-RAG
References
Improving RAG Answer Quality Through Complex Reasoning was originally published in Towards Data Science on Medium, where people are continuing the conversation by highlighting and responding to this story.
Originally appeared here:
Improving RAG Answer Quality Through Complex Reasoning
Go Here to Read this Fast! Improving RAG Answer Quality Through Complex Reasoning